The report of the Bhore Committee (headed by Sir Joseph William Bhore) in 1946 came up with the first blueprint for a tax-funded health system in India with primary healthcare as its core. In 1978, India endorsed the WHO’s Declaration of Alma-Ata, which proclaimed an explicit commitment to comprehensive primary healthcare as a state responsibility, and in 1983, the country’s first National Health Policy was crafted with the goal of providing “Health for All by 2000 through comprehensive PHC Services”. Yet, India’s healthcare system seems to have fallen short of the hoped-for transformation. Instead, we have a highly privatised healthcare sector with sharp rural-urban imbalances in terms of access, personnel distribution, and treatment.
According to the January 2026 report of “The Lancet Commission for a citizen-centred health system for India”, the people have a fundamental and inalienable right to health and the government must be accountable for financing and operating public sector healthcare and provide stewardship for private sector healthcare. It is also the commission’s understanding that the conventional barriers to universal health do not exist any more as they are no longer driven by a lack of political will, underfunding, inadequate human resources and physical infrastructure, or low demand for healthcare services.
The real challenges now are uneven quality of care, uneven and inefficient spending, fragmented delivery, inadequate design and implementation of financial protection programmes, and poor governance, according to the commission. Drawing on a wide range of expertise, the commission’s latest report calls for an integrated healthcare delivery system that is publicly financed as the primary vehicle for universal health coverage, while shaping the private sector to leverage its strengths.
There is little doubt that India has made remarkable progress in life expectancy, infant and maternal mortality, and control of infectious diseases. But progress has been uneven across States and districts. There are wide variations in the provision of health services between States and even within individual States. Similarly, there are wide variations between income groups, social groups, marginalised castes, tribes, and genders. Non-communicable diseases, mental health conditions, and antimicrobial resistance pose a different set of challenges.
Undeniably, there has been considerable improvement in healthcare access. Government initiatives—such as Ayushman Bharat-PradhanMantri Jan Arogya Yojana (AB-PMJAY), Ayushman Arogya Mandirs, and Ayushman Bharat Digital Mission e-Sanjeevani telemedicine platform—and the deployment of medical cadre and allied medical health professionals, new tertiary hospitals and medical colleges, and an expanding private sector have made medical services available to a greater number of people.
But, the commission argues, uneven quality of healthcare has limited the value of expanded access and of care in general. The fault lines are therefore in the conceptualisation and implementation of primary healthcare, which has fallen short of meeting people’s needs. Without care coordination, citizens are left to fend for themselves and receive care of uncertain quality from myriad providers, often at expensive hospitals rather than in primary healthcare facilities, undermining continuity, equity, and efficiency.

A health camp in an interior village in Alluri Sitharama Raju district of Andhra Pradesh, where many tribal children suffer from sickle cell anaemia, a file photograph. | Photo Credit: K.R. DEEPAK
At a leading private hospital with multiple branches in the national capital, nursing staff and some medical personnel told this correspondent that managements in private hospitals often put pressure on their staff to meet targets. “There is competition between branches to see which branch raises more revenue. The consultation fee for the same doctor can vary depending on the location of the branch. The more upscale the area, higher the consultation fee,” said one healthcare provider formerly associated with the hospital.
Doctors who do not prescribe a certain number of tests are less likely to rise in the system. While medical personnel receive fixed salaries, their pay package includes a component similar to what is called a “performance linked incentive” in the private sector.
Patients from the rural hinterland seek medical care in the metros, increasing work pressure on nursing staff, medical personnel, and non-medical staff in city hospitals. With contractual employment, hospitals frequently lose staff to competitors. All this does not make for healthy commitment to patients.
The commission’s report noted that government spending on health has increased in absolute terms but remains low as a proportion of the GDP; that means, it has not kept pace with the country’s economic growth. Rigid public budgets and fee-for-service payments in the private sector reduce the system’s ability to adapt to population needs and provide appropriate, cost-effective care.
Limitations of insurance schemes
While insurance and financial inclusion schemes like the AB-PMJAY have expanded, insurance schemes are by and large still focussed on hospitalisation, ignoring outpatient and chronic care. As a result, out-of-pocket expenditures are high.
White-collar employees have access to quality healthcare, thanks to higher incomes and corporate insurance cover. But for the majority of the working class and lower-income groups, accessing private-sector multi-speciality hospitals remains out of the question and awareness of insurance schemes is low. Still, people with lower incomes try to access healthcare by mortgaging assets like land or jewellery.
Consider this scenario at a leading private hospital in Delhi. A patient who had to undergo a critical surgery was assured of a bed a week before the procedure. An advance payment for the procedure and the bed had been made at the hospital’s booking desk. The understanding was that the patient would admit herself the previous evening and undergo the preoperative tests and check-ups. When she arrived at the scheduled time, she was told that no bed was available and she could take a refund if she wanted. She also noticed that there were obviously well-heeled people waiting to be allotted beds.
At a primary healthcare centre in Tirunelveli, Tamil Nadu, a file photograph. Serious illnesses often force citizens to seek treatment in expensive hospitals rather than in primary healthcare facilities. | Photo Credit: A. SHAIKMOHIDEEN
Close to midnight and a few hours before the operation, she was allotted a bed in a room that had another occupant. After the surgery, she was wheeled into the room. The next day, the security guard on the floor told her that she could collect her discharge papers, which were ready. In other words, she had to vacate the room, ostensibly for another patient in queue. This was the state of a multi-chain private hospital group in the national capital.
Private sector accounts for bulk of outpatient consultations
According to the commission, India’s private sector accounts for the majority of outpatient consultations and also substantially for inpatient care. This sector, it says, must be leveraged as the country’s partner in the universal health coverage journey.
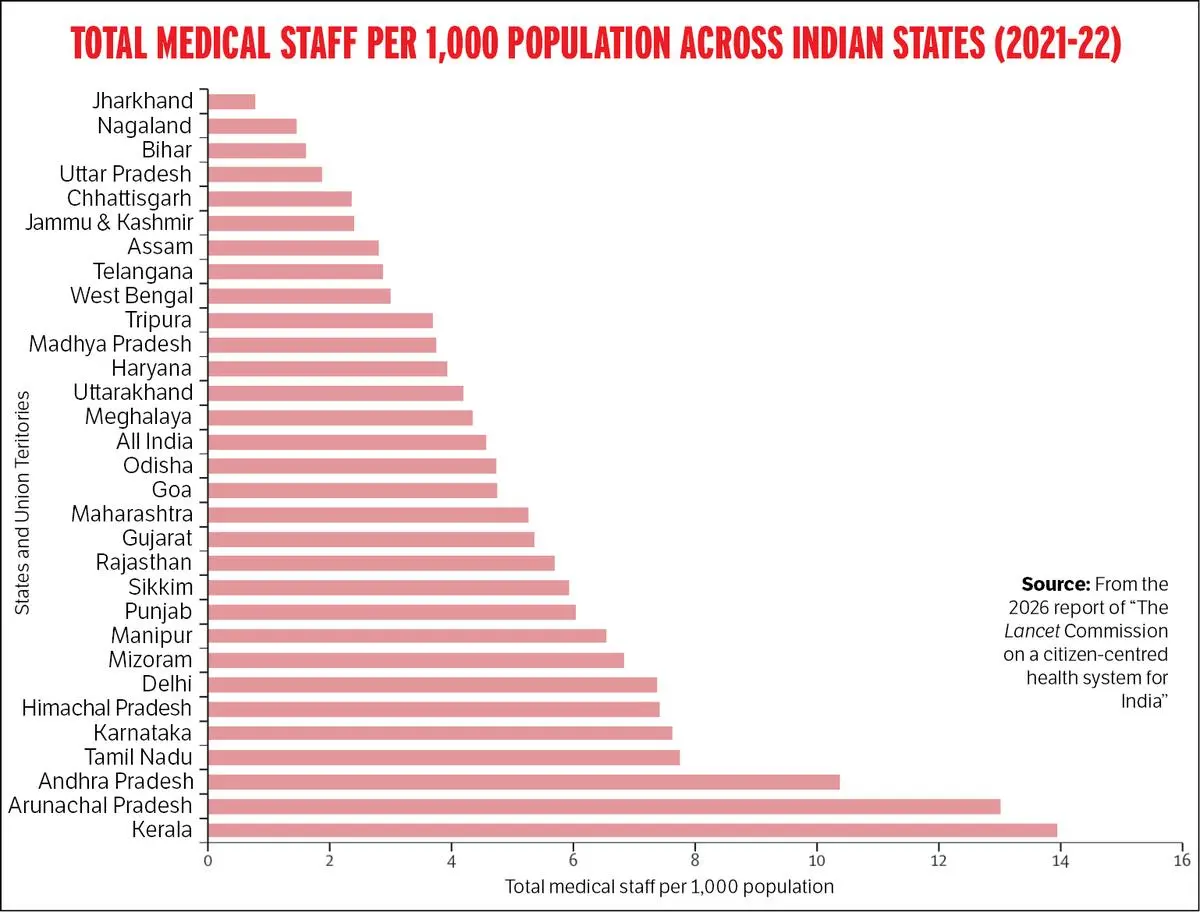
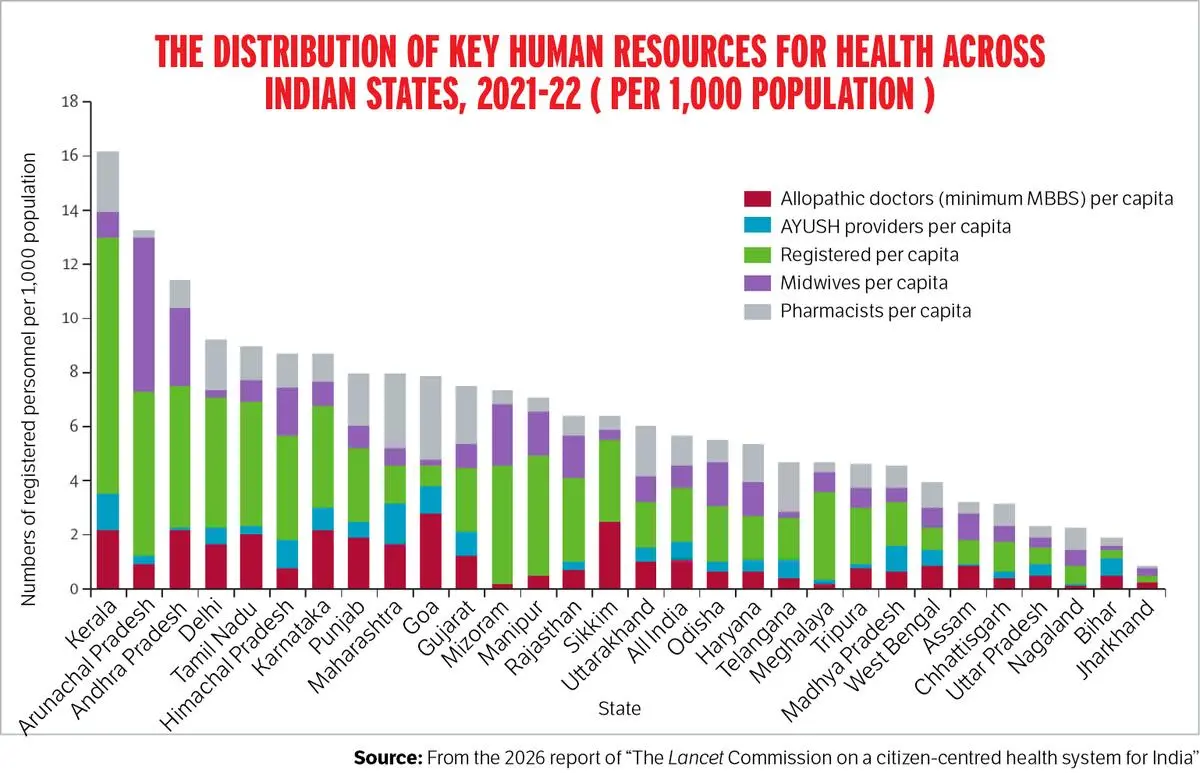
As for public sector healthcare facilities, there are considerable variations in the range of services offered across States and districts. A 2021 government study quoted in the commission’s report noted that inter-State variations in district hospitals ranged from 1 to 408 beds for every 1,00,000 people. The ratio of doctors, as per the norms of the Indian Public Health Standards (IPHS), was highest in Haryana (1.42) and lowest in Uttarakhand (0.48). In Tamil Nadu, while district hospitals fulfilled 16.8 per cent of IPHS-recommended functional specialities, only 1 per cent of these specialities were available in Assam, Goa, Punjab, Madhya Pradesh, Mizoram, and Uttar Pradesh. Primary health centres (PHCs) in Bihar and Jharkhand had a 70 per cent shortfall of MBBS doctors, whereas States such as Maharashtra, Telangana, and Arunachal Pradesh had between one and a half and five times the required number of MBBS doctors.
The largest proportion of private sector facilities, says the commission, are small units like single-provider clinics, nursing homes with fewer than 10 beds, or stand-alone diagnostic centres, all operating with limited staff. The larger corporate hospitals, which represent a much smaller fraction of facilities, contribute disproportionately to tertiary care capacity.
Many such hospitals follow a “hosted model” where specialist doctors and surgeons practise independently on the hospital premises, supported by the hospital’s infrastructure, nursing staff, and diagnostic facilities. While this model allows for flexibility and access to a wider range of expertise, it can result in variability in clinical quality and care coordination. This, the commission says, also poses challenges for stronger referral linkages, interoperable health records, and quality assurance mechanisms to ensure consistency across the care continuum.
More medical personnel with expansion in medical education
There has been a substantial increase in the number of medical personnel. In 2023–24, the doctor to population ratio was 1:1,263. If Ayush physicians were included, this was 1:834, an increase of 40 per cent since 2010. The corresponding ratio for nurses and midwives was 2.89 for 1,000 people, below the WHO norm of 4 nurses and midwives for 1,000 people.
The number of doctors increased due to the expansion in medical education through new training institutions, expanded intake capacity of existing medical institutions, upgrading of district hospitals to medical colleges, and relaxations in norms for setting up nursing institutions and medical colleges in the private sector.
The bulk of India’s qualified health workforce is employed in the private sector: 65 per cent of MBBS doctors, 93 per cent of Ayush physicians, 51 per cent of nurses, and 67 per cent of other providers. The majority of providers, 73 per cent of all MBBS doctors, were in urban areas. An estimated 43 per cent of the total stock of health providers are not adequately qualified.
In contrast, as of March 2022, 24 per cent of the sanctioned posts of doctors were vacant in public-sector PHCs; so were 68 per cent of specialist posts at community health centres and 85 per cent of posts of doctors and specialists across public-sector hospitals and subdivisional hospitals.
Women registering for free screening for breast and cervical cancer at a camp organised by the Indian Medical Association, in Karnataka’s Ballari. | Photo Credit: THE HINDU ARCHIVES
Around 25 to 40 per cent of doctors and specialists were absent from work at public sector primary care facilities, whereas 20 to 50 per cent of the doctors engaged in dual practice (legally allowed by some States) while holding public sector jobs. Worryingly, the benchmark for sanctioning health personnel in public sector facilities does not take into account workload and staffing needs, which leads to skewed distribution even when positions are filled.
There is also skewed distribution between States. In 2019, only 27 per cent of MBBS doctors and 36 per cent of nurses worked in rural areas, where 65.5 per cent of India lives. A huge cadre of community health workers (1.08 million), the Accredited Social Health Activists, serve as the first point of contact in the public healthcare system. But they are recruited on a voluntary basis and entitled to an honorarium instead of regular wages with attendant benefits. The Central government has not accepted their demand to be treated as government employees.
Notwithstanding improvements in availability of services, tribal people continue to lag behind in accessing healthcare. In 2018, a study (quoted in the commission’s report) found that 82 per cent of vulnerable tribes sought healthcare when ill against 92.5 per cent of the general population.
Compared with city residents and high-income groups, low-income groups and rural residents fare poorly in terms of accessing antenatal care, institutional deliveries, and immunisation. There are considerable gaps in access to surgical procedures and secondary and critical care among districts, especially in the least developed and north-eastern States.
In 2019, there were 1,385 surgeries for 1,00,000 people; the WHO benchmark is 5,000 surgeries for 1,00,000 people. In critical care workforce and infrastructure, the shortfall was an acute 90 per cent. A 2023 survey by the Transform Rural India Foundation found that 57.7 per cent of households migrated out of their home districts to seek hospital treatment for serious ailments, whereas 36.7 per cent sought such care because of better facilities elsewhere, outside their home districts.
The authors of The Lancet Commission’s paper assert that while services for chronic conditions have improved, access to citizen-centric care is missing. Illnesses in lower-income households go undiagnosed for long periods and are detected only when complications set in, leading to higher healthcare costs and poor outcomes.
While screening for major chronic diseases showed an almost 29-fold surge between 2019–20 and 2025–26, a nationwide facility readiness study showed that only 1.1 per cent of rural public sector facilities and 9 per cent of urban private sector facilities at the primary level have all the essential technologies and medicines to manage non-communicable diseases. This means that people have to travel long distances to access treatment for chronic diseases.
A radiologist working in a well-known private hospital told this correspondent that he shifted there recently from a government cancer institute in the capital as diagnostic services and equipment were either not available or not of the requisite standard. “It’s a pity. Hundreds of patients come to the institute, and we didn’t have the equipment to do the necessary procedures. We deal with technology. If that is not available, no point hanging around. I left because of that,” he said.
The Transform Rural India Foundation Survey found that only 13.8 per cent of respondents reported having access to diagnostic services at their primary care facility. Most diagnostic services were purchased in private hospitals or private laboratories. The Citizens’ Survey (2023) found that, nationally, two-thirds of families bypassed primary care facilities in the public sector to seek care from private hospitals. Studies have found that 90 per cent of medicines are bought from the private sector, adding to out-of-pocket expenditure.
For a developing country like India, the public sector should be the principal provider of healthcare in order to ensure equity, with the private sector playing a supportive and complementary role. Instead, we have a healthcare system tilted in favour of those who can afford it.
Also Read | Workplace as death-trap
Also Read | Patriarchy’s health wreck needs women in charge now
Also Read | A promise lost in fine print