Women spend more of their lives in poor health than men. Despite this inequity, we have the potential to add seven more days of healthier life per woman per year – a pursuit that would require a combination of improved research, efficacy and care.
A new report from the World Economic Forum's Global Alliance for Women’s Health in collaboration with the McKinsey Health Institute (MHI) builds on the finding that care delivery constitutes 34% of the women’s health gap. Gaps in care deliver entail from inequities, including missed screenings, delayed diagnoses and inconsistent treatment. Closing this care delivery gap is both a moral imperative and an opportunity.
The Global Alliance for Women’s Health and MHI modelled the impact of these care inequities at national levels. This study found that closing these gaps could avert around 70,000 adverse events such as heart attack, heart failure, stroke and more, every year in the US alone. For women, this translates into better quality of life – equivalent to around 2.5 additional healthy days each year.
Investing in preventive care such as integrated screenings and standardized reporting could create healthcare system savings, delivering a 3–6x return on investment by shifting from costly downstream events to preventive care: a check up and early intervention is much cheaper than a medical emergency.
The implications are systemic. Previous research shows that closing gaps in women’s health could contribute at least $1 trillion annually to global GDP by 2040, driven by improved health, workforce participation and productivity. Improving care delivery – and outcomes for women – is among the most actionable ways to create this value.
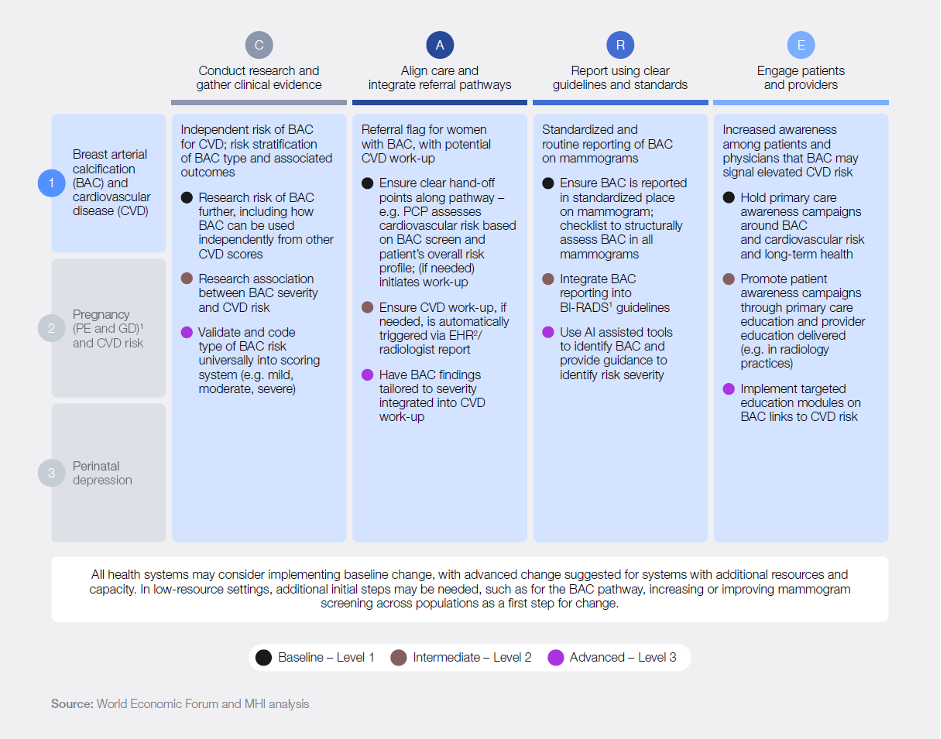
Closing this gap goes beyond science. It also requires applying what already works. The CARE framework offers a practical way to do that:
C: Conduct research and gather clinical evidence – developing additional evidence and research needed to implement solutions.
A: Align care and integrate referral pathways – care pathways are fragmented and need to be aligned across practices.
R: Report using clear guidelines and standards – there is a lack of standardized reporting and integration of guidelines across pathways.
E: Engage patients and other health system stakeholders in patient-centred care – patient-centric care and provider-level awareness are needed to address challenges.
At its core, the CARE framework is about closing the gap between what health systems know and what they do in practice. By adopting this framework, health systems and providers can do their share to improve the healthspan and lifespan of women worldwide.
The Forum and MHI's report brings this to life through three high-impact care pathways, where gaps are both meaningful and solvable.
The first is breast arterial calcification (BAC) – detectable during routine mammograms – is an indicator of cardiovascular risk. Today, this signal is often overlooked, but embedding BAC assessment into standard practice could enable earlier intervention and prevent adverse events such as heart attacks and strokes.
Preventive care triggered by BAC identification costs about $500 per woman and delivers a 3–5x return by preventing costly downstream events using existing mammography systems. Scaling this approach across the US could avert 17,000-60,000 cardiovascular events over seven years, averting a spend of $2–$3.5 billion with prevention costs of just $700 million to $1.5 billion.
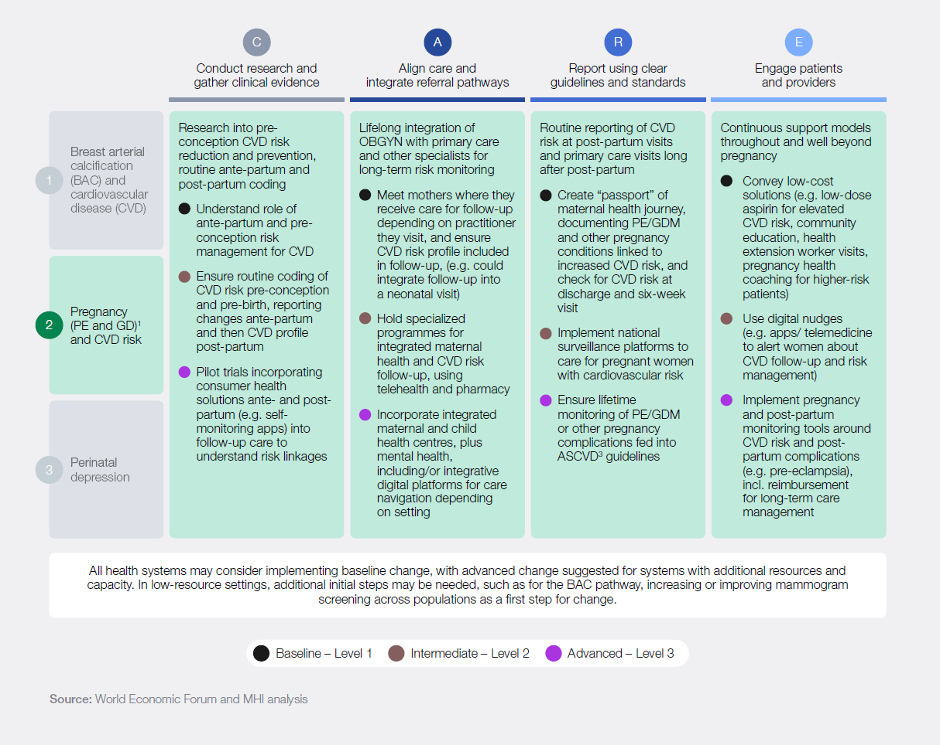
A second critical pathway is pregnancy and cardiovascular disease risk. Conditions such as pre-eclampsia and gestational diabetes are well-established predictors of long-term cardiovascular disease, but they are rarely integrated into ongoing cardiovascular risk assessment after pregnancy. As a result, many women miss the chance for early monitoring and preventive care,.
Improving follow-up and long-term care costs about $400–$450 per woman – far lower than the $100,000–$120,000 cost of treating major cardiovascular events. In the US alone, this could avert approximately ~$6–$25 million in avoided costs from $1.5–$4 million investment over 15 years, delivering roughly a 3-5x return.
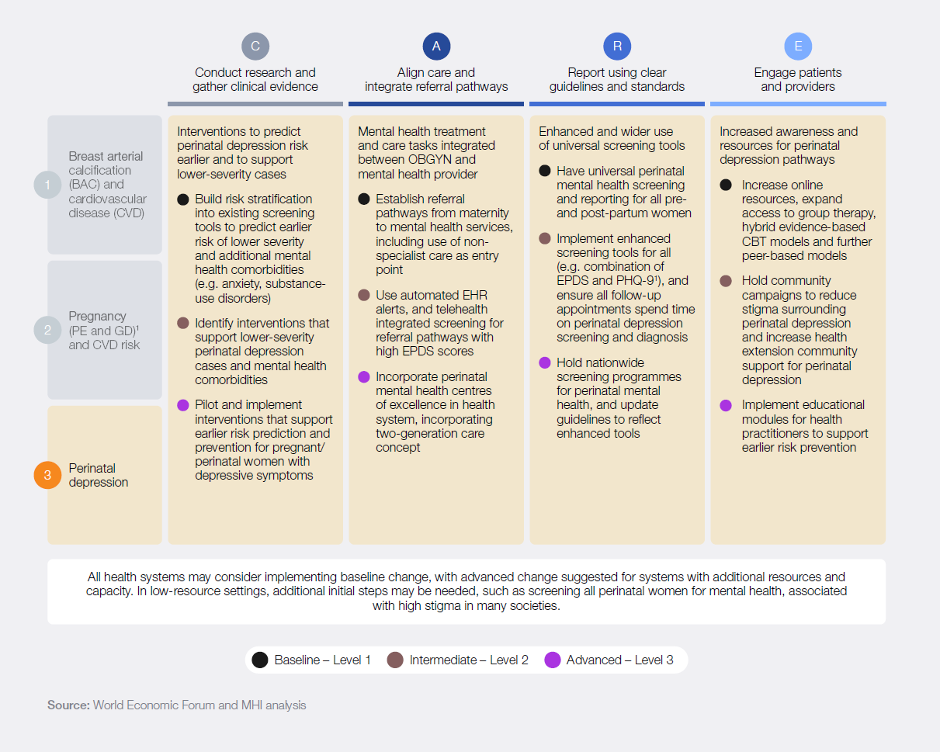
The third pathway, perinatal depression, underscores a different but equally urgent challenge. Affecting around one in five women, perinatal depression remains widely under-diagnosed and under-treated, despite the availability of validated screening tools and effective interventions.
Because the perinatal period is foundational for both maternal health and early child development, failures in care can have lasting consequences – not only for mothers, but for their children as well. Perinatal depression–related adverse events cost ~$250–$700 million in the US.
Realizing this potential will require coordinated action across the health ecosystem. Providers, payers, governments, regulators, innovators and patients each have a role to play in redesigning care pathways that reflect women’s needs across the life course. Encouragingly, many of the required changes build on existing infrastructure – from enhancing screening protocols to strengthening referral systems and improving follow-up care.
The roadmap provides clear, practical pathways tailored to different levels of complexity, enabling every health system to take meaningful steps – whether by integrating new screening markers, improving care coordination or strengthening follow-up protocols. With this roadmap, health systems can start moving from insight to implementation.
By adopting and scaling these approaches, healthcare providers can begin redesigning care pathways within their institutions, helping to avert thousands of preventable cases while improving outcomes for women and unlocking significant economic gains.
此内容由惯性聚合(RSS阅读器)自动聚合整理,仅供阅读参考。 原文来自 — 版权归原作者所有。